

ABOUT CLEFT lip and palate
A cleft lip is a split in the upper lip, a cleft palate is a split in the roof of the mouth. They occur during early development in the womb, when the upper lip or palate doesn’t join together properly.
Cleft lips or palates occur in 1 in 600 to 1000 births, making it one of the most common major birth defects. Clefts occur more often in kids of Asian, Latino, or Native American descent.
The three common kinds of clefts are:
- cleft lip without a cleft palate
- cleft palate without a cleft lip
- cleft lip and cleft palate together
In addition, clefts can occur on one side of the mouth (unilateral cleft) or on both sides of the mouth (bilateral cleft).
The good news is that both cleft lip and cleft palate are treatable. Most kids born with these can have reconstructive surgery within the first 12 to 18 months of life to correct the defect and significantly improve facial appearance.
DEVELOPMENT OF A CLEFT LIP OR PALATE
Each of us had a cleft lip and cleft palate during the early weeks of development in our mother’s womb. Normally, the tissues that form the palate (the roof of your mouth) and the upper lip come together in the middle and join (fuse). You can see the lines of fusion in the “Cupid’s bow” under your own nose, and feel the ridge and line in the middle of your palate (the roof of your mouth). If your baby has a cleft, this fusion did not happen when he or she was developing.
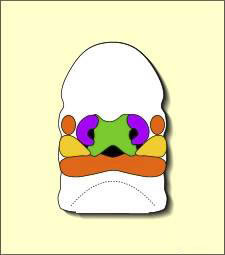
Embryo at 7 weeks
During the first six to eight weeks of pregnancy, the shape of the embryo’s head is formed. The lips and palate originate from three areas of the baby’s developing face. These areas are also called prominences. They are the Central or “Frontal Nasal” prominence (green in the illustration), the Left “Maxillary” prominence (yellow), and the Right “Maxillary” prominence (yellow). The Central prominence will grow and become the infant’s forehead, nose, middle portion of the upper lip (called the philtrum or Cupid’s bow) and the primary palate, which is the part of the upper jaw that holds the middle four teeth. The Left and Right “Maxillary” prominences will grow and become the lower face, the lower lip and jaw (all but the middle portion of the upper lip and jaw), and the “secondary” palate (this is the part of the palate from behind the middle four upper teeth to the back of the mouth).

Embryo at 10 weeks
If these tissues fail to meet, a gap appears where the tissues should have joined (fused). This may happen in any single joining site, or simultaneously in several or all of them. This is what we call a cleft lip or cleft palate
ABOUT THE CAUSES OF CLEFT LIP AND PALATE
In most cases, we simply don’t know why lip and palate development go wrong.
Race and gender play a small role. Cleft lips and palates are most common in Asians. They are less common in Caucasians and least common in African people. Boys are more often affected than girls.
In some families, cleft lip and palate appear in several family members, so heredity is important. Sometimes substances in the environment, called teratogens, may be associated with clefts. But most babies with clefts have no known relatives with cleft lip or palate and no known exposure to teratogens. A few babies with cleft lip and palate also have other abnormalities.
CLEFT LIP SURGERY
Cleft lip is formed in the top of the lip as either a small gap or an indentation in the lip (partial or incomplete cleft) or continues into the nose (complete cleft). Cleft lip can occur as one sided (unilateral cleft lip) or two sided (bilateral cleft lip).
Partial unilateral cleft Complete unilateral cleft Bilateral cleft
A mild form of a cleft lip is a microform cleft. A microform cleft can appear as small as a little dent in the red part of the lip or look like a scar from the lip up to the nostril. In some cases muscle tissue in the lip underneath the scar is affected and might require reconstructive surgery. It is advised to have newborn infants with a microform cleft checked with a craniofacial team as soon as possible to determine the severeness of the cleft.
In general, patients with clefts have a deficiency of tissue and not merely a displacement of normal tissue.
SURGICAL ANATOMY
Before describing some of the characteristics of a cleft lip and its repair, it helps to be familiar with some of the common landmarks and anatomy of a normal lip. Cupid’s bow is central to the upper lip, with its peaks delineating the philtrum between the philtral columns.
NORMAL LIP ANATOMY
The demarcation between mucosa and skin of the lip is called the vermilion border. The mucosa or vermilion of the lip is further divided into dry and wet sections. The protuberant vermilion in the midline is referred to as the tubercle. The two nostrils (nares) are separated by the columnella externally and the septum internally.
Below the surface, the orbicularis oris muscle encircles the oral aperture, creating a sphincter. The fibers decussate in the midline creating the philtrum. In the cleft lip, the orbicularis muscle inserts into the nasal alar base.
Lip musculature. A) Normal musculature with fiber decussation to form the philtral columns. B) Cleft musculature with abnormal muscle insertions into the base of the nose.
CLEFT LIP SURGERY
Cleft lip often requires only one reconstructive surgery, especially if the cleft is unilateral. Cleft lips are repaired at about 2-3 months of age. It is carried out under full anesthetic.
Bilateral cleft lips may be repaired in two surgeries, about a month apart, which usually requires a short hospital stay.
The basic goal of cleft lip, alveolus, and palate repair, whether for the unilateral or bilateral anomaly, is to restore normal anatomy. The objectives of surgical repair of the cleft lip are two-fold: restore aesthetic ‘normal’ landmarks and reconstruct a functional orbicularis oris. There are many variations in the technique of cleft lip repair.
The repair involves making incisions and bringing the pieces of lip together to form a full lip. There are a number of different techniques from which the surgeon can choose depending on the nature of the cleft. Two of the most common approaches are the rotation-advancement and the triangular flap repair.